



Cognitive Behaviour Therapy (CBT)
“People are not disturbed by things, but by the view they take of them” (Epictetus, Greek philosopher)
What is cognitive behavioural therapy (CBT)?
CBT is a talking therapy and a well-recognised psychological treatment that research suggests is likely to be helpful for a number of difficulties (e.g. depression and anxiety).
Although we cannot always change or control the type of life situations that may cause us psychological distress, we can change how we respond to these situations to reduce the level of psychological distress we may experience. CBT attempts to change a person’s response to life experiences by using various methods to help a person change their thinking.
What do many of us believe about the cause of our feelings and behaviours?
When you ask people what has upset them, they generally start by describing ‘what happened’ to them (i.e. they tell us about a specific situation). For example, “I am so annoyed because my partner does nothing to help around the house, so I have to do everything which always makes me late for work”.
Most of us share the belief, at some level, that it is ‘what happens’ in a specific situation that is mainly responsible for how we actually feel or behave at that time. This seems to make good sense as whenever you find yourself in a particular situation you may often seem to find yourself responding (feeling or acting) in the same kind of ways.
For example, whenever you find yourself in situations where people are treating you unfairly you are likely to feel angry or upset and may act in a way that reflects this (e.g. argue, complain, walk away, etc.). So it seems reasonable to expect that, over time, we may naturally come to believe that it is a ‘specific situation’ that ‘makes us feel or act’ in a particular way. This is called the ‘common sense’ model of human behaviour because most of us share this belief at some level and it seems to be true of our life experiences.
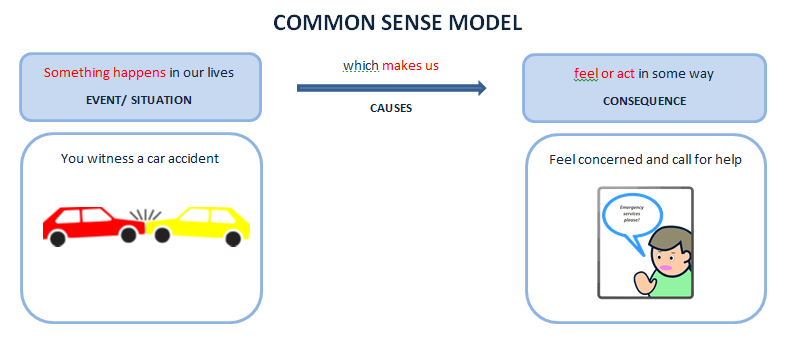
In time we may take this idea to its logical conclusion, to believe that only if the ‘situation’ (what happens to us) changes then our feelings and the way we act will change. Again this seems to make good sense and we often find ourselves and others understandably saying things like, “I wouldn’t be angry all time if my partner did their share of the work around the house”.
However, although this view of human behaviour seems to make sense to us, we all probably suspect at some leve that it isn’t quite that simple. For one, it does not take us long to realise that this view of our world does not always make sense, for a number of reasons:
Firstly, if we believe that it is the situation itself (‘what happens’) that causes us to feel and act in certain ways then we should find, in our own lives and in the lives of others, that we/they always feel and act in exactly the same way in similar situations. However, we all know that we don’t always respond to similar situations in our own lives in the same way nor do others respond to the same situations we are a part of in the same way. For example, are you likely to respond to exactly the same rude comment from a parent, partner, child, close friend or boss? In situations where you find yourselves with other bystanders, do they all respond exactly in the same way as you do?
Secondly, even when we manage to avoid or change the situation that upsets us, we may find that the upset still remains or that it is not long before we find ourselves upset in a similar way by other situations.
Is what we ‘think’ about a situation responsible for our response to it?
So it would seem that the situations we find ourselves in, on their own, do not cause us to feel or behave in specific ways. If this were true, then a specific situation (event) should automatically cause everyone who experienced it, to feel and behave in exactly the same way. However, what we see in our everyday lives is that, to a greater or lesser extent, people respond differently to the same or similar events. This is even true of very traumatic situations (events) people experience (e.g. death of a loved one, being diagnosed with a fatal disease, etc.), as some people manage to cope reasonably well while others do not. However, if the ‘common sense’ model is not able to fully explain our behaviour, what model would?
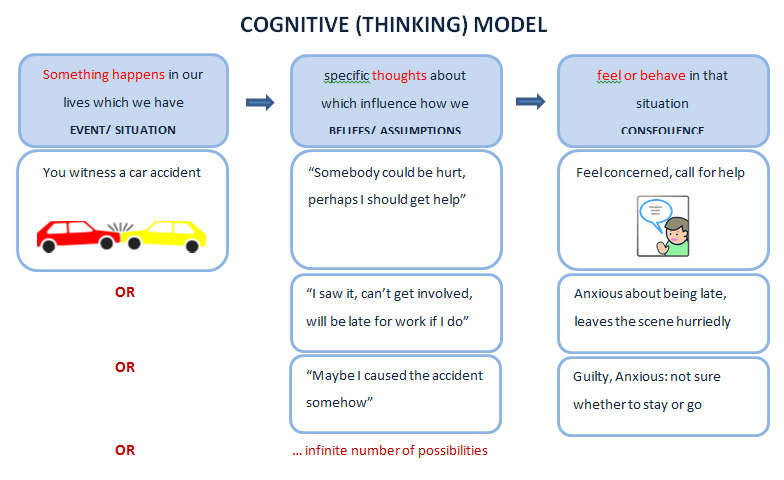
One model which may be able to better explain our behaviour is the model that cognitive behavioural therapy (CBT) is based on, called the ‘cognitive’ model. The word ‘cognitive’ comes from the word ‘cognitions’ which simply refers to our ‘thinking’ which would include the assumptions and beliefs we have about ourselves, others and things in life in general. This model argues that, it is not the situation (event) itself that causes us to feel or behave in certain ways, but rather ‘what we think’ about the situation (i.e. the meaning we give to it) that will strongly influences how we are likely to feel and behave in that situation.
This model would better explain why people witnessing the same event may respond similarly or differently, as it would all depend on the way they are interpreting the event (i.e. how they are thinking about it) at the time. According to this model, those that have similar thoughts about the event will have similar emotional or behavioural responses whereas those who don’t won’t.
In the same way it would explain why we ourselves may respond differently to similar events in our lives because we would be telling ourselves different things at the time (e.g. if your partner was rude to you over the phone and thought that it was undeserved, you may clearly show your annoyance with him/ her by hanging up. However, in exactly the same situation with your boss on the phone, although you may feel annoyed you may also be telling yourself that you really need this job and don’t think you can afford to offend your boss, so you endure your annoyance and don’t hang up. The only difference is what you told yourself. However, if you told yourself in both situations that nobody gets to talk to you like that then you would have probably hung up in both situations).
References
Westbrook, D., H. Kennerley & J. Kirk, (2011) An Introduction to Cognitive Behaviour Therapy: Skills and Applications 2nd Edition. SAGE Publications, London.
 |
Appointments±
Fees±
Standard appointment: (50-60 minutes)
- £75 (self paying clients)
- £90-120 (health insurance)
First appointment: (120 minutes)
- £150 (self paying clients)
- £180-240 (health insurance)
Should additional time or a brief report be required, it is charged pro-rata of the standard appointment rate.
Payment options±
Payment can be made by:
- Cash (paid at the appointment)
- Bank transfer (BACS, paid before the appointment)
- Health insurance (claimed directly from your insurer)
To pay by health insurance you will first need to check that your provider pays for our services, then provide your health insurers name, your policy number and the authorisation code (claim number) before booking an appointment.
Crisis/ emergency information±
This practice does not offer a mental health crisis or emergency service. If you feel extremely distressed and and in need of urgent care (e.g., have suicidal thoughts and fear you may harm yourself, or feel that you may be a danger to others), please seek immediate medical assistance.
For NHS information: dealing with a mental health crisis or emergency please click here. It discusses possible options to consider depending on your situation, such as:
- follow your mental health team’s advice, if you are under their care (such as a Crisis Resolution and Home Treatment Team (CRHTT))
- telephone an NHS helpline: phone 111 (urgent care) or 999 (emergency care)
- go to your local hospital's 'accident and emergency' (A&E) department
- contact your medical doctor (GP) for an emergency appointment
- call Sussex Mental Health Line, phone 0300 5000 101
- call The Samaritans who operate a free to call service 24 hours a day, 365 days a year, phone 116 123
Services±
Assist adults (at least 20 years old) with:
- Anxiety (e.g., post-traumatic stress (PTSD), generalised anxiety (GAD), health anxiety, panic, social anxiety, obsessive-compulsive disorder (OCD), phobias)
- Low mood (e.g. feeling sad or depression)
- Adjusting to significant life events (e.g., the end of an important relationship)
- Loss and bereavement (i.e., grief)
- Low confidence or self-esteem
- Impact of dysfunctional parenting in childhood focusing on emotional neglect and the relationship difficulties and unhelpful relationship patterns that result from this
Although I work with clients having difficulties concerning their important personal, family and/or work relationships, I do not offer couple / marital / family counselling.
Services not offered:
- Child, family, couple/marital counselling
- Forensic (psycho-legal) assessments/ reports for expert witness
- Some mental health difficulties (e.g., eating disorders, psychotic disorders, drug or alcohol addictions, personality disorders)
Treatments±
Psychotherapies or interventions offered:
- Cognitive behaviour therapy (CBT)
- Person centered therapy (Rogerian)
- Brief Psychodynamic therapy
- Transactional analysis therapy (TA)
- Relaxation training
- Basic mindfulness
- Psycho-education
Other information±
Registrations and supervision:
- BPS registered (chartered status)
- HCPC registered (counselling psychologist)
- Data Protection (ICO Registered)
- Supervised by a DPsych, BABCP, HCPC & BPS accredited psychologist
Practice summary information±
Guy Suter | Chartered Psychologist | HCPC Registered
Independent psychologist in private practice offering a psychotherapy service for adult clients (20+) in Crawley, Horsham and East GrinsteadThree Bridges
Crawley
West Sussex
United Kingdom
RH10 1SQ
Click to phone
Click to email
Monday – Friday | 09:00–17:00
Monday - Thursday | 17:00-20:00
Closed public holidays